
Why Heat Matters in Orthopedic Surgery
Introduction: The Paradox of Heat in Bone Surgery
In bone surgery, heat is both a tool and a threat. Controlled energy enables precise cutting, drilling, and fixation, yet excessive heat can damage living bone, jeopardize implant stability, and delay osseointegration.
Research shows that bone exposed to temperatures above approximately 116.60°F (47°C) for more than one minute can sustain permanent osteocyte injury and protein denaturation, leading to localized necrosis [1]. The challenge for surgeons and engineers alike is finding ways to harness energy safely, delivering enough to anchor or shape bone without crossing into thermally destructive territory.
The Science Behind Thermal Stress in Bone
Traditional fixation techniques, such as drilling, reaming, or cement polymerization, generate heat at the bone surface. Even purely mechanical insertion methods can produce brief temperature spikes in the cortical layer, sufficient to impair local microcirculation.
Thermal insult initiates a cascade of biological changes: osteocyte apoptosis, microcrack formation, and delayed mineralization along the remodeling front.
Experimental work demonstrates that short exposures near 122°F (50°C) can reduce early bone-to-implant contact and delay new bone formation; across studies, critical thresholds for necrosis are reported between 116.60°F (47°C) and 131°F (55°C) if exposed for more than one minute [1, 4].
Figure 1: Mechanism Of SupraFusion Technology. The SupraFusion Technology uses ultrasonic liquefaction to anchor implants directly into bone.
Understanding the Role of Ultrasonic Energy
Ultrasound-assisted fixation, as used in the SupraFusion system, applies vibrational energy to the thermoplastic interface between the implant and the bone.
Rather than relying on mechanical torque, ultrasonic energy briefly liquefies a thin polymer layer, which then flows into trabecular pores and solidifies within milliseconds, creating a tight, three-dimensional interlock.
The key variable is temperature control, how much the bone heats, how rapidly it cools, and how deeply the heat penetrates. SupraFusion technology is engineered to confine the heating zone to the implant interface, protecting the surrounding cortical and cancellous bone.
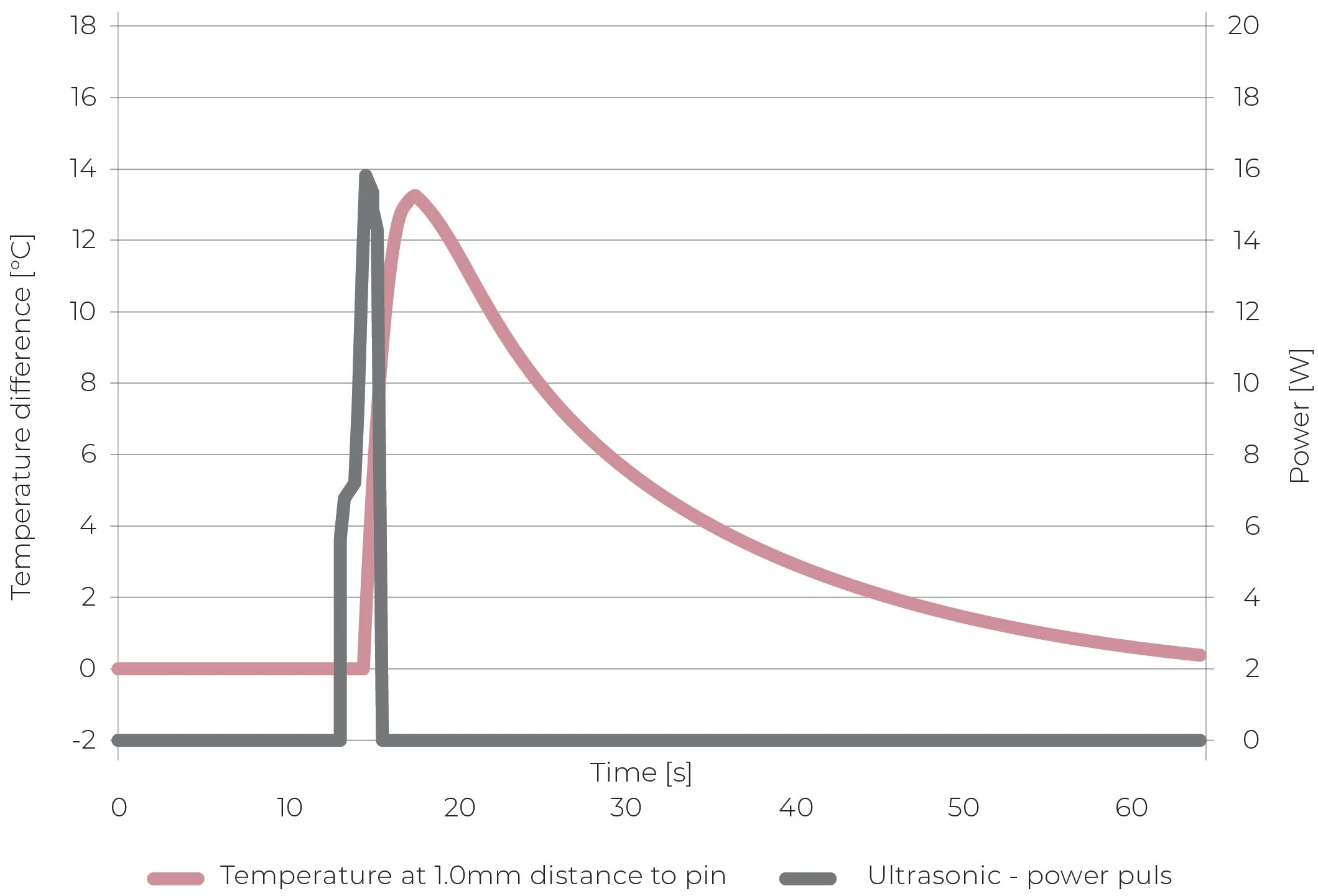
Figure 2: In Vivo Thermal Curve Recorded During Ultrasonic Fixation. SupraFusion Technology uses brief ultrasonic energy to soften the implant’s surface, without compromising bone biology.
Evidence from Preclinical Research
Pre-clinical studies conducted by the Musculoskeletal Research Unit (MSRU) at the University of Zürich confirm that ultrasound-assisted polymer anchoring maintains safe thermal margins and supports bone vitality.
The average temperature rise was about 46.4-55.4°F (8-13°C) for a few seconds, and the temperature at 60s post-insertion was +35.6°F (+2°C) which is well below necrotic thresholds.
Histology revealed no bone necrosis, no capsule formation, and low scores of inflammatory cells, and new mineralized bones were observed directly adjacent to the implant surface [2, 3].
Ground-section histology demonstrated direct bone contact with the polymer interface, without fibrous tissue interposition, even in zones corresponding to maximal heat exposure.
These findings indicate that short, localized, sub-threshold heating does not compromise interfacial bonding and early bone remodeling when thermal exposure is properly controlled.
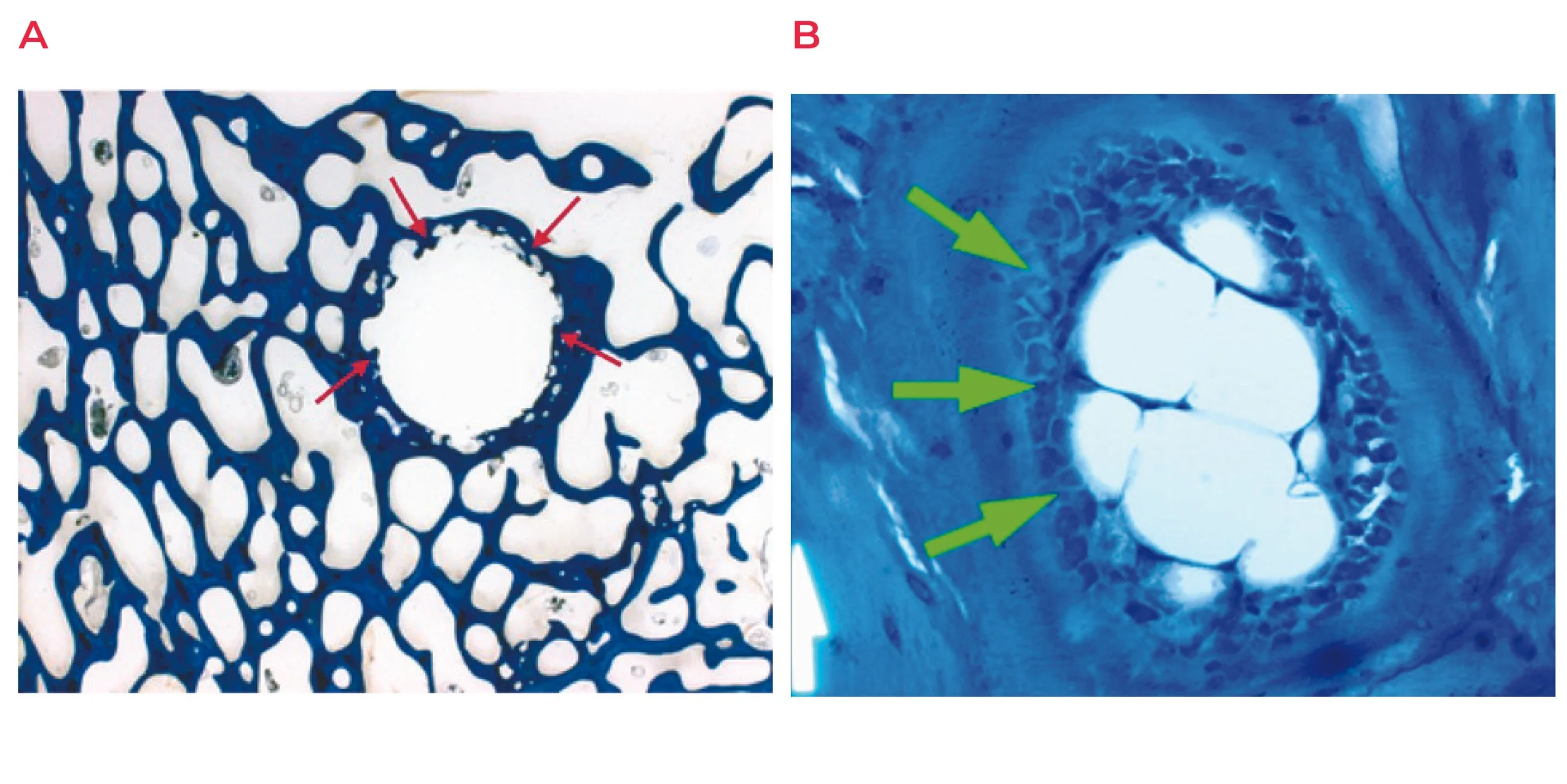
Figure 3: Histological Analysis Of The Bone. 6 months post-op with homogenous osteointegration with the polymer (labeled arrows show bone growing into polymer) without signs of osteolysis (a). New bone formation (green arrows) by osteoblasts around the polymer (b).
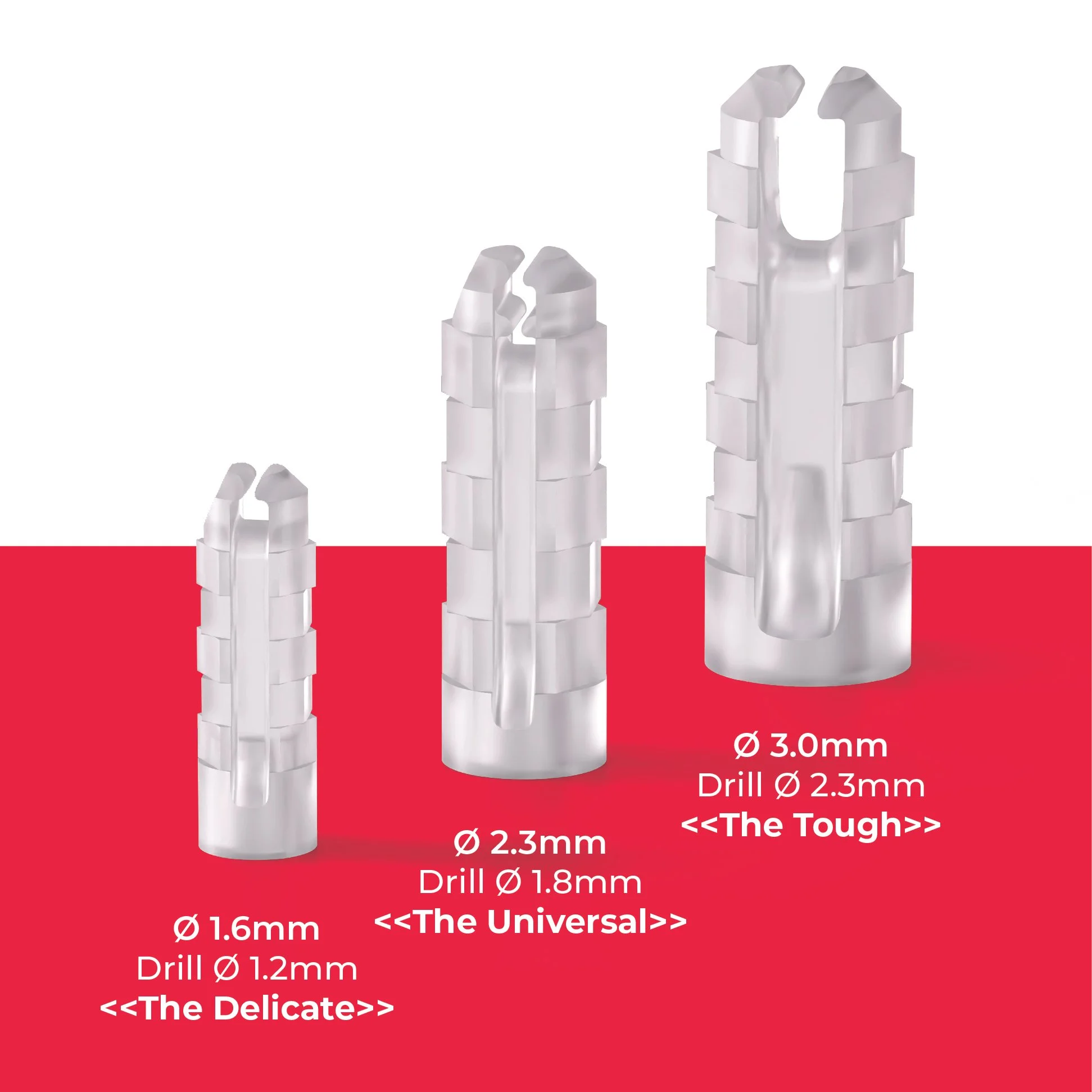
Figure 4: SupraFusion Push-in Anchor Portfolio. The SF Push-in Anchor Portfolio provides 3 implant sizes.
SupraFusion’s Thermal-Friendly Advantage
SupraFusion’s proprietary ultrasonic system transforms energy-assisted fixation into a thermally friendly anchoring effect, in which heat, flow, and stability occur as a single controlled event. By modulating amplitude and exposure duration, the system creates only a brief, localized temperature rise that remains within a safe temperature range [2, 3]. This short, confined pulse softens the polymer just enough to interdigitate with the surrounding bone while preserving osteocyte vitality, an outcome consistently confirmed by histology, which shows no thermal injury or inflammation.
Because the system relies on small, precisely delivered implants, it naturally fits the tight anatomical spaces of the hand and wrist. The reduced implant size minimizes bone removal, lowers surgical trauma, and decreases the volume of tissue requiring repair, all of which complement the gentle thermal profile. As the polymer resolidifies, immediate mechanical stability is achieved without disrupting the biological environment needed for regeneration.
In this way, SupraFusion uses ultrasonic energy as a regenerative ally, strengthening the bone-implant interface while protecting the very cells responsible for long-term healing.
Surgical Takeaway
In orthopedic fixation, heat defines the boundary between safe integration and biological compromise. SupraFusion’s thermally intelligent process demonstrates that brief, localized, and self-limiting heating does not compromise bone–implant integration. On the contrary, it provides outstanding performance. Combined with its small footprint, precise placement, and low-trauma insertion, the system offers an important advantage for surgeons treating challenging indications, especially in the tight, delicate corridors of the hand and wrist.
References
1. Chen Y-C, Tsai Y-J, Hsiao H-Y, Chiu Y-W, Hong Y-Y, Tu Y-K, Hsiao C-K, et al. Assessment of thermal osteonecrosis during bone drilling using a three-dimensional finite element model.Bioengineering (Basel). 2024;11(6):592.
2. Langhoff JD, Kuemmerle JM, Mayer J, et al. An ultrasound-assisted anchoring technique for fixation of implants to bone: a histological pilot study in sheep.Open Orthop J. 2009;3:40–47.
3. Heidenreich D, Langhoff JD, Nuss K, et al. The use of BoneWelding technology in spinal surgery: an experimental study in sheep.Eur Spine J. 2011;20(11):1821–1836.
4. Augustin G, et al. Cortical bone drilling and thermal osteonecrosis.Int Orthop. 2012;36(4):755–760.