
When Millimeters Matter: Fixation in Tight Anatomy
Introduction – The Challenge of Small Bone Fixation
In the small bones of the hand, wrist, foot, and ankle, fixation must be performed within tight corridors of bone where every millimeter matters. Traditional threaded implants carve through this limited bone stock, creating expanding cones of stress that restrict how close implants can be placed and often pull surgeons away from ideal anatomic reconstruction. These constraints arise not from surgical biology, but from the mechanical demands of thread-cutting hardware [1].
The Engineering Problem Inside Small BoneS
Small-bone anatomy leaves little margin for error: thin cortices, narrow volumes of cancellous bone, and high risk of tunnel collision. Threaded implants remove bone and generate overlapping stress fields when placed too closely. In many reconstructive procedures in tight spaces in the hand & wrist and foot & ankle, this forces the surgeon to compromise fixation patterns to accommodate implant spacing rather than anatomy [1].
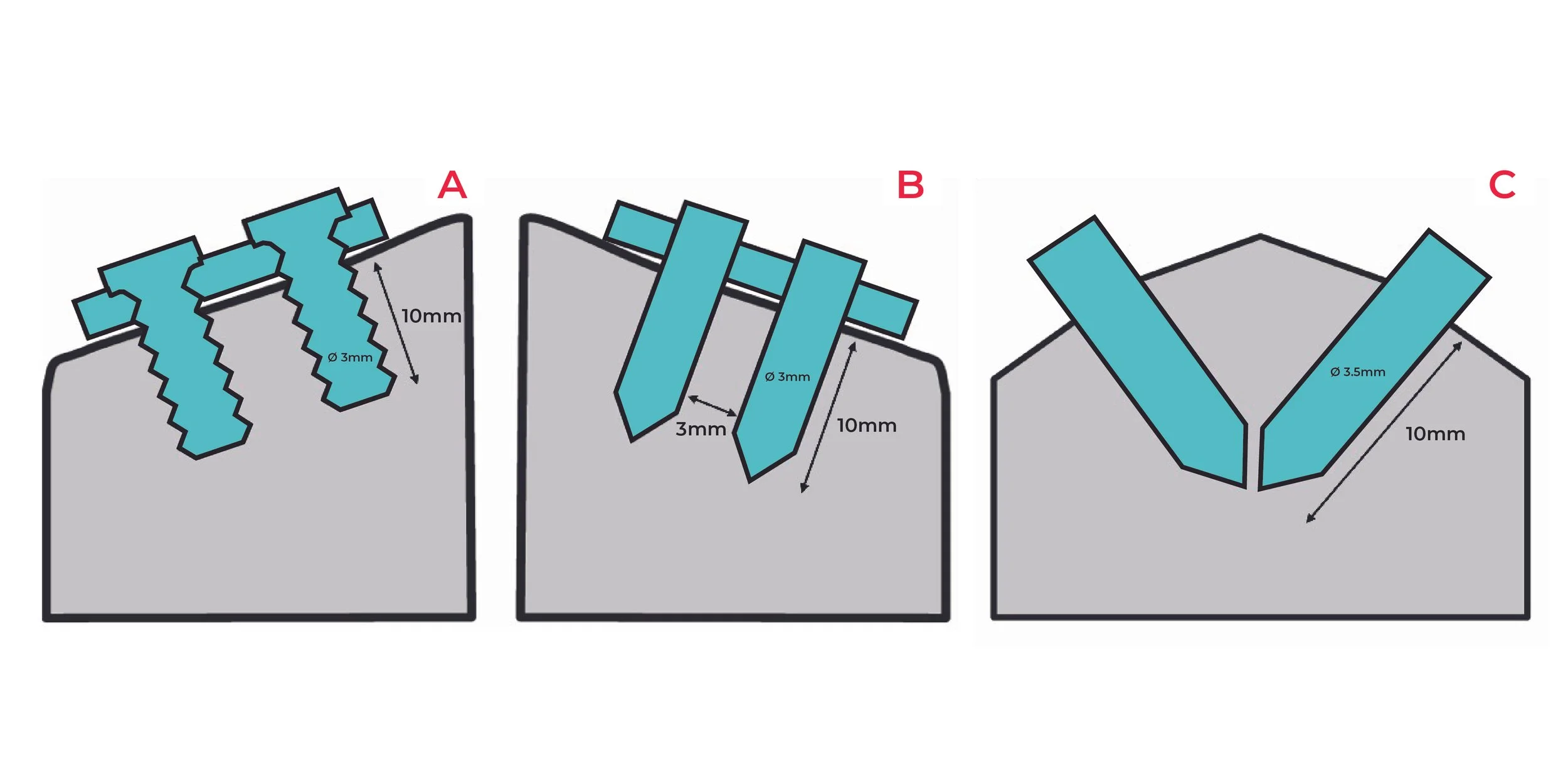
Figure 1: Overview Of Surgical Configurations. (a) Parallel PLDLLA Screw (Ø 3.0mm), (b) Parallel PLDLLA SupraFusion (Ø 3.0mm), (c) Converging PLDLLA SupraFusion (Ø 3.5mm). Parallel PLDLLA Screw (a) and Parallel PLDLLA SupraFusion (b) were secured with a plate. In all configurations, the implants were inserted 10mm into the bone [2].
How We Tested Fixation in Tight Anatomy
To determine whether dense fixation could be performed safely, researchers recreated the smallest and most challenging anatomical scenarios in pre-clinical studies. Three configurations were tested as shown in Figure 1:
· Parallel PLDLLA screw as control (Figure 1a)
· Parallel PLDLLA implant inserted using SupraFusion Technology (Figure 1b)
· Converging PLDLLA pair whose tips approached within ≤ 1mm of each other and inserted through SupraFusion Technology (Figure 1c)
All implants were placed 10mm deep with bone bridges of ~ 3mm, conditions that mirror real small-bone anatomy [2]. The studies assessed bone-to-implant contact, inflammatory response, radiology, microradiography, and thermal behavior.
A Different Biological Interface: Interdigitation, Not Cutting
SupraFusion Technology uses brief ultrasonic energy to soften a thin PLDLLA surface, allowing it to flow into natural trabecular pores before solidifying. This creates immediate 360° interdigitation, without removing bone [1][2].
Histology showed direct bone contact, active osteoblasts, controlled remodeling within ~ 1mm, and no fibrous capsule formation, indicating a healthy biological response [1][2].
What Evidence Shows: Bone Safety Even Millimeters Apart
Parallel Implants (~ 3 mm apart)
Even with minimal spacing, the trabecular bone between implants stayed intact. Figure 2 radiographical images showed continuous bone architecture with no necrosis or voids [2].
Converging Implants ( ≤ 1 mm apart)
In the most challenging condition, cancellous bone remained healthy. No cystic change, resorption, inflammatory infiltration, or structural compromise was observed (Figure 2) [2].
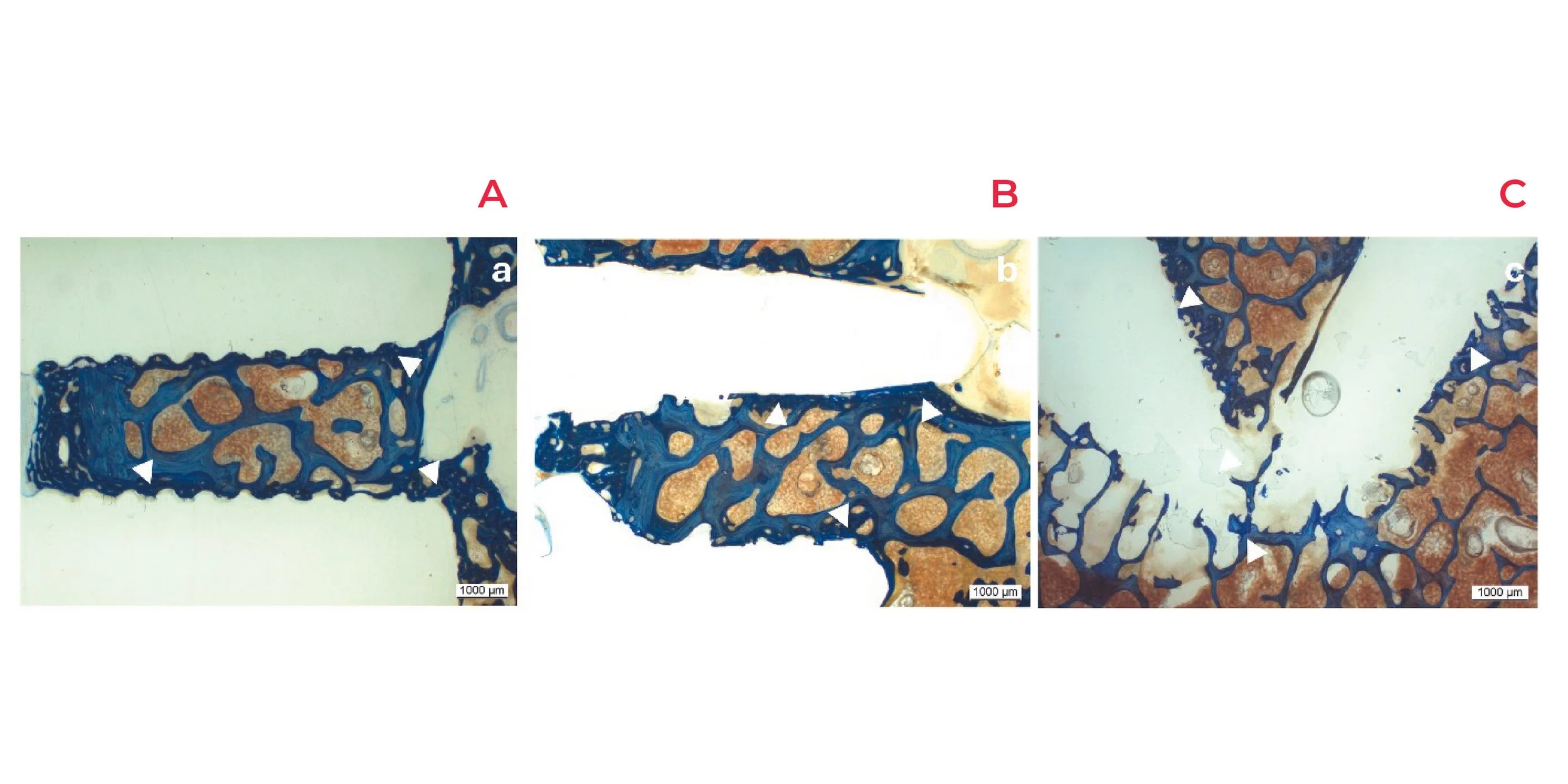
Figure 2: Overview Of Histological Section. Parallel PLDLLA Screw (a), parallel PLDLLA SupraFusion (b), and converging PLDLLA SupraFusion (c), at 2 months post-implantation. Direct contact between new woven bone (white triangle) and implant surface, with the absence of fibrous capsule formation at 2 months post-implantation and across all configurations.
Inflammatory Response and Bone RemodelinG
Inflammatory cell scores remained below 1.5 across all groups, with new woven bone forming directly on the implant surface and no fibrous capsule formation. Remodeling stayed localized and controlled, indicating a calm biological response [2].
Radiographic Stability
Radiographs at 2 months showed stable implants with preserved trabecular continuity and no signs of bone damage [2].
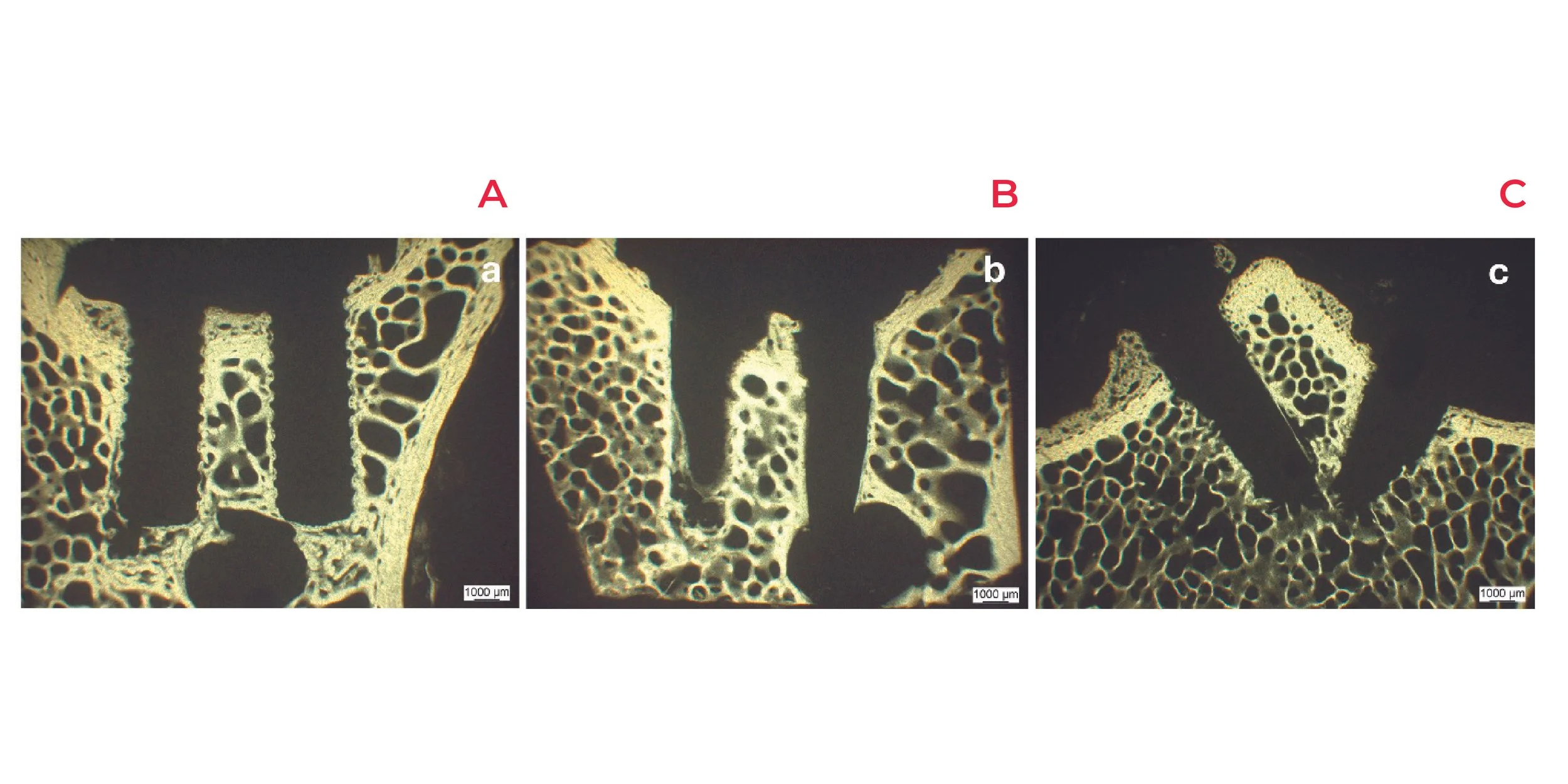
Figure 4: Radiological Image After 2 Months Of Implantation. Parallel PLDLLA Screw (a), parallel PLDLLA SupraFusion (b), and converging PLDLLA SupraFusion (c) remained well-positioned, without signs of bone damage or changes related to fixation technology.
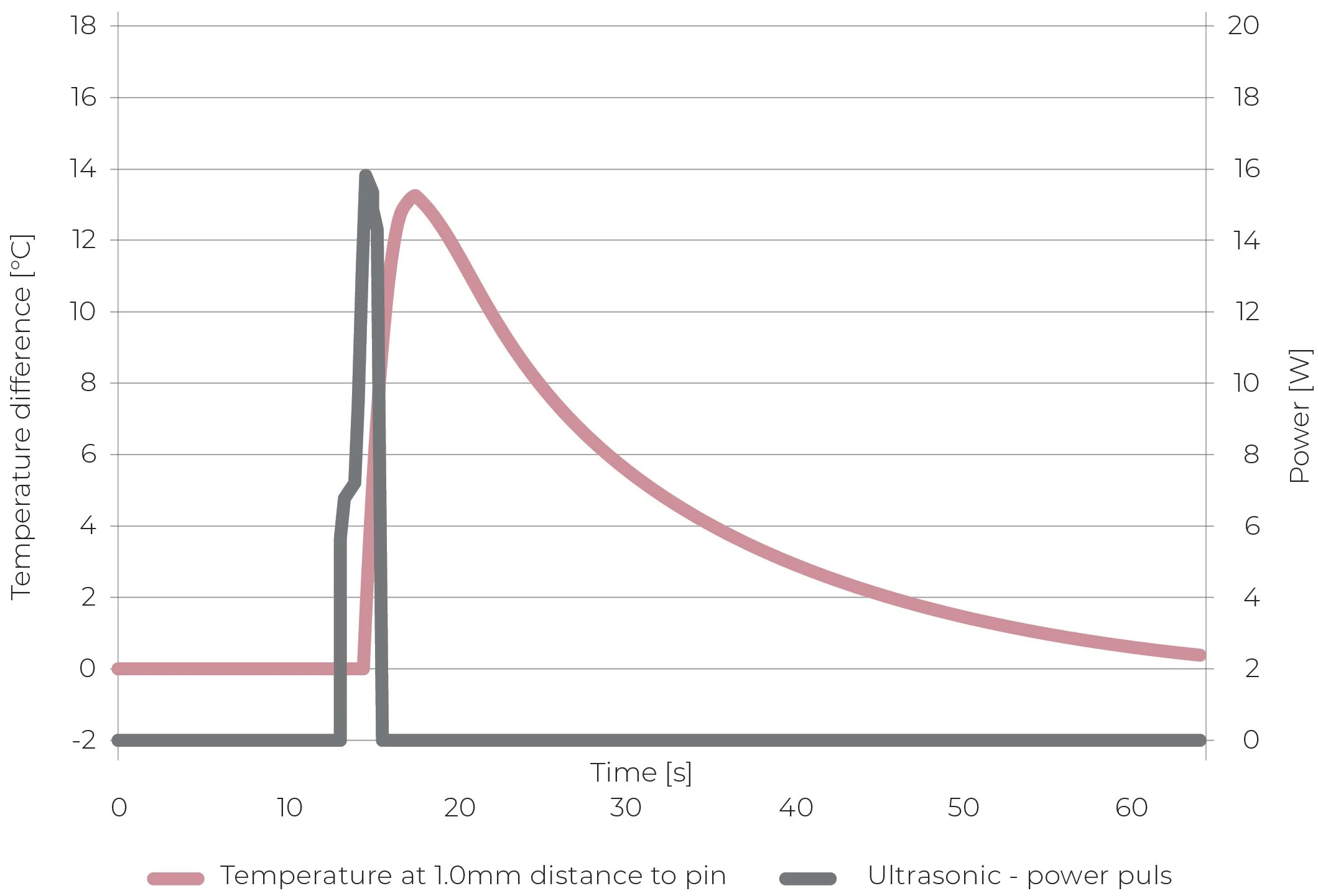
Figure 5: In Vivo Thermal Curve Recorded During Ultrasonic Fixation. SupraFusion Technology uses brief ultrasonic energy to soften the implant’s surface, without compromising bone biology.
Thermal Safety During Insertion
A common concern with ultrasonic activation is heat. In vivo thermocouple recordings showed a peak temperature increase of 46.4 - 55.4°F (8 - 13°C), lasting < 1 second, well below thresholds known to injure bone. This thermal exposure was also lower than conventional drilling procedures [2].
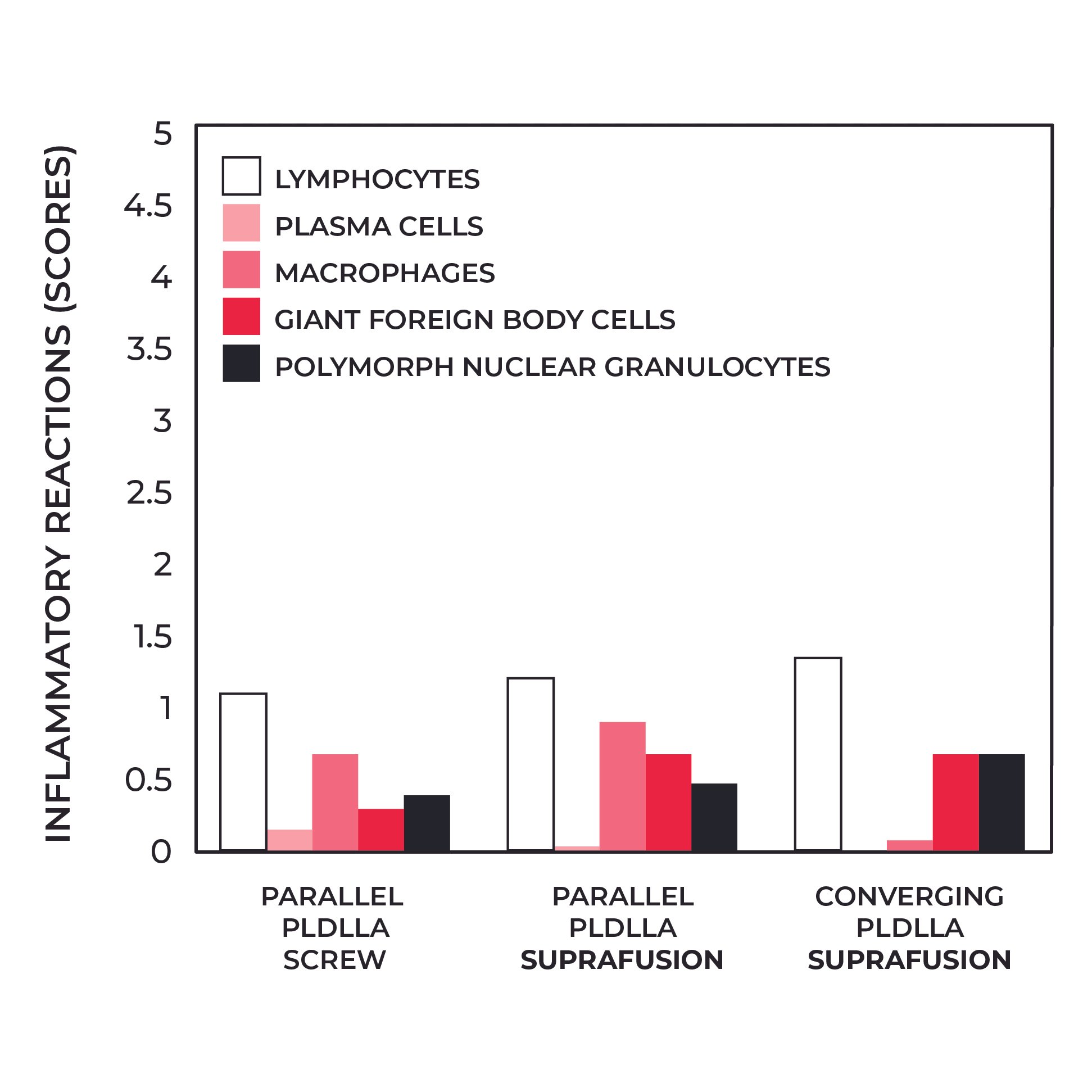
Figure 3: Inflammatory Cell Reactions. After 2 months, inflammatory cell scores remained below 1.5 for all groups. Even when two SupraFusion implants were inserted at minimal distances, the inflammatory response remained low.
Why This Matters in Surgery
Dense fixation is essential for restoring anatomy in small joints, especially in the hand & wrist and the foot & ankle. Thread-cutting devices impose spacing rules that anatomy does not allow. A bone-preserving method allows fixation to follow the biology of the repair rather than the mechanics of the implant [1, 2].
SupraFusion Technology: Enabling Fixation Where Space Is Limited
SupraFusion Technology preserves bone structure, enabling anchors to be placed only millimeters apart, even along converging paths. Pre-clinical studies consistently show intact bone bridges, low inflammation, predictable remodeling, and safe thermal exposure across challenging configurations [1, 2].
When every millimeter matters, fixation can finally be guided by anatomy, not hardware limitations.
Key Takeaway
PLDLLA implants fixed with SupraFusion Technology demonstrate safe, stable, bone-preserving performance even when placed extremely close together. This opens the door to truly anatomic fixation strategies in the smallest bones of the extremities.
References
1. Langhoff JD, Kuemmerle JM, Mayer J, Weber U, Berra M, Mueller JM, et al. An ultrasound-assisted anchoring technique for fixation of implants to bone: A histological pilot study in sheep.Open Orthop J. 2009;3:40–47.
2. Heidenreich D, Langhoff JD, Nuss K, Kluge K, Kämpf K, Zlinszky K, et al. The use of ultrasound-assisted polymer anchoring technology in spinal surgery: an experimental study in sheep. Eur Spine J. 2011;20:1821–1836.
3. Spine Study on sheep, 2010. Data on record.