
Skier’s Thumb Under Pressure: Achieving Stable Fixation in the Smallest Bones
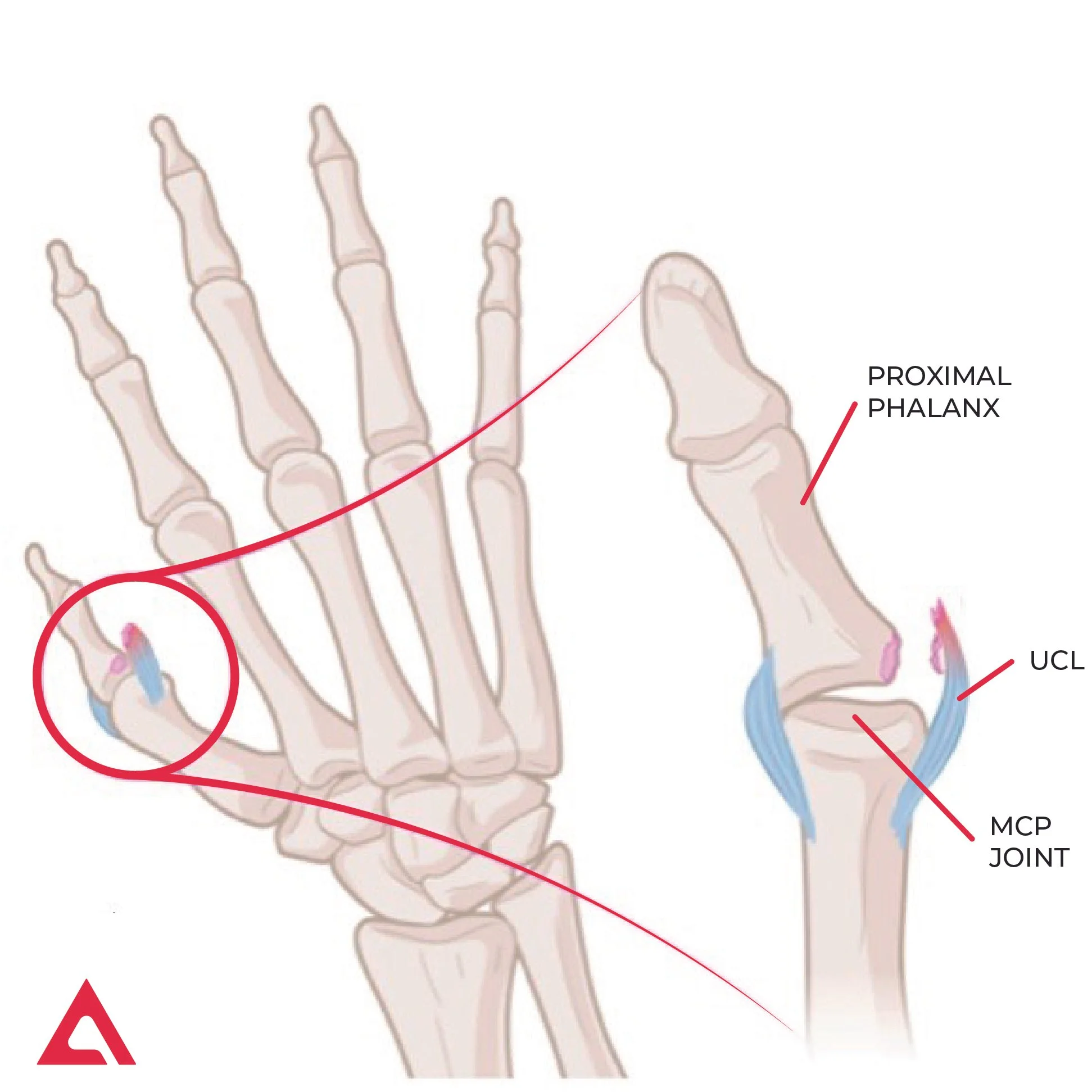
Figure 1: Anatomy Of Skier's Thumb. Ulnar collateral ligament (UCL) injury at the metacarpophalangeal (MCP) joint.
Introduction — Why This Injury Demands Precision
Skier’s thumb, an ulnar collateral ligament (UCL) injury of the metacarpophalangeal (MCP) joint, is one of the most common hand injuries in alpine sports. Caused by a sudden valgus force on the abducted thumb, often during a fall while gripping a ski pole, this injury challenges surgeons because it combines high functional demands with the bone’s small, delicate anatomy.
In a skier’s thumb injury, surgical repair is recommended to restore joint stability. However, achieving reliable fixation in the thumb’s cancellous bone, often with limited cortical support, remains technically demanding.
Background & Science — Understanding the Fixation Challenge
Anatomy and Injury Mechanism
The thumb MCP UCL is the primary stabilizer against valgus stress. When ruptured, spontaneous healing is unlikely. Surgical reattachment of the ligament to the proximal phalanx is therefore recommended in displaced injuries (> 3mm) to restore stability and prevent chronic weakness or pain.
Why Small Bone Matters
Unlike larger joints, the proximal phalanx of the thumb offers:
Limited bone stock
Predominantly cancellous bone
Often incomplete or compromised cortical support, e.g., due to a cortical bone chip that broke away with the ligament’s failure
Traditional fixation strategies frequently rely on larger anchors or cortical engagement, which may not be optimal in this anatomical context. The challenge is not simply fixation strength but strength relative to implant size, achieved without further compromising the bone.
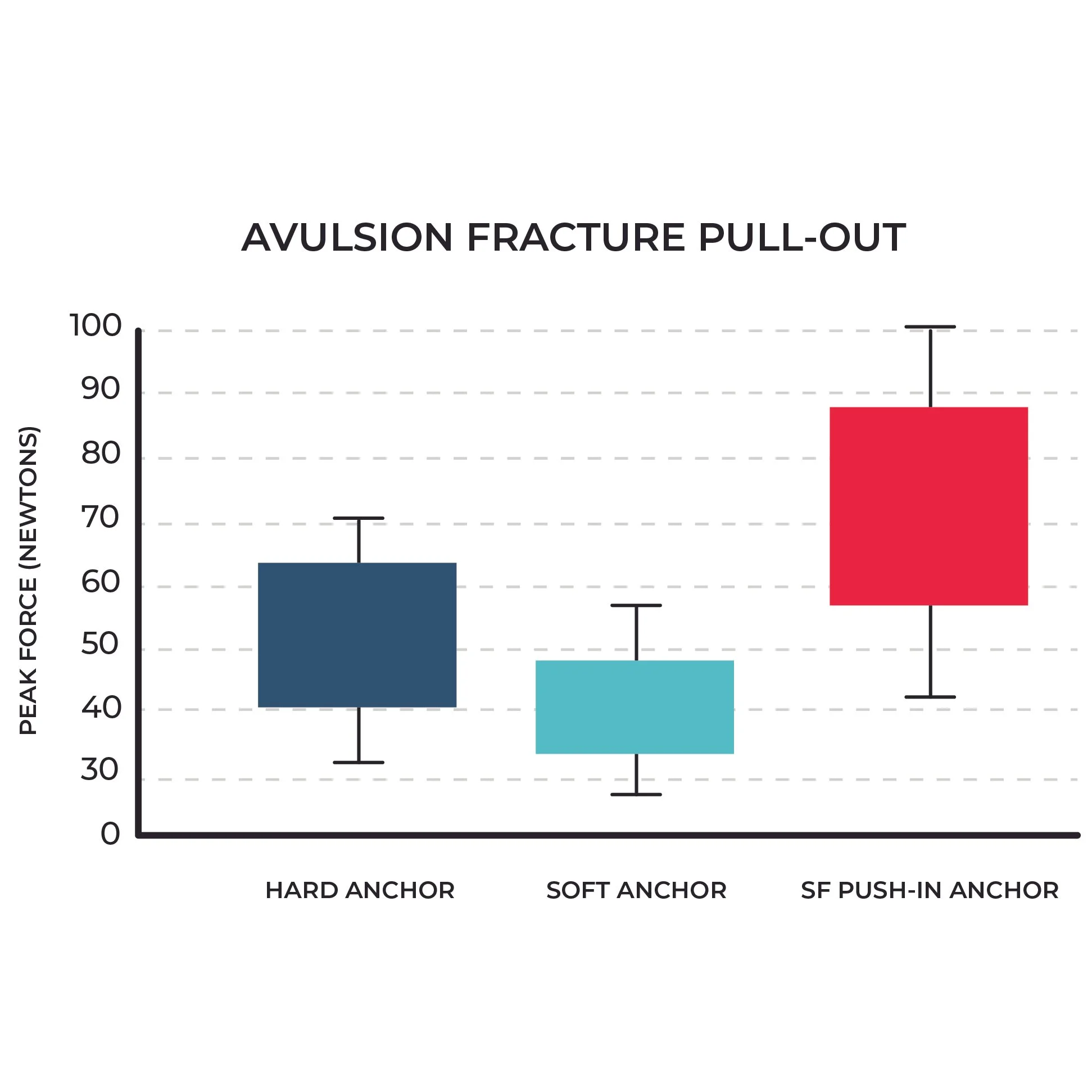
Figure 2: Pullout Force Comparison Of Different Suture Anchor Systems In Thumb UCL. The graph shows that the SF Push-in Anchor requires the greatest force to pull out, indicating the highest strength among the 3 anchors.
Biomechanical Requirements for Thumb UCL Repair
For athletes and high-demand patients, fixation must tolerate early functional loading while maintaining ligament apposition. Key biomechanical requirements include:
Stable anchorage in cancellous bone
Resistance to pullout without reliance on an intact cortex
High strength-to-size efficiency
In a controlled biomechanical comparison, Wagner et al. evaluated suture anchors for thumb UCL repair and demonstrated that an ultrasonically anchored polymer implant achieved high pullout forces despite a markedly smaller diameter compared with conventional anchors (Figure 2). Because this implant is fixed by ultrasonic integration into cancellous bone, as seen in Figure 3, rather than by mechanical expansion or cortical purchase, the results highlight how the mode of bone–implant interaction, not implant diameter alone, contributes to fixation strength in small bone.
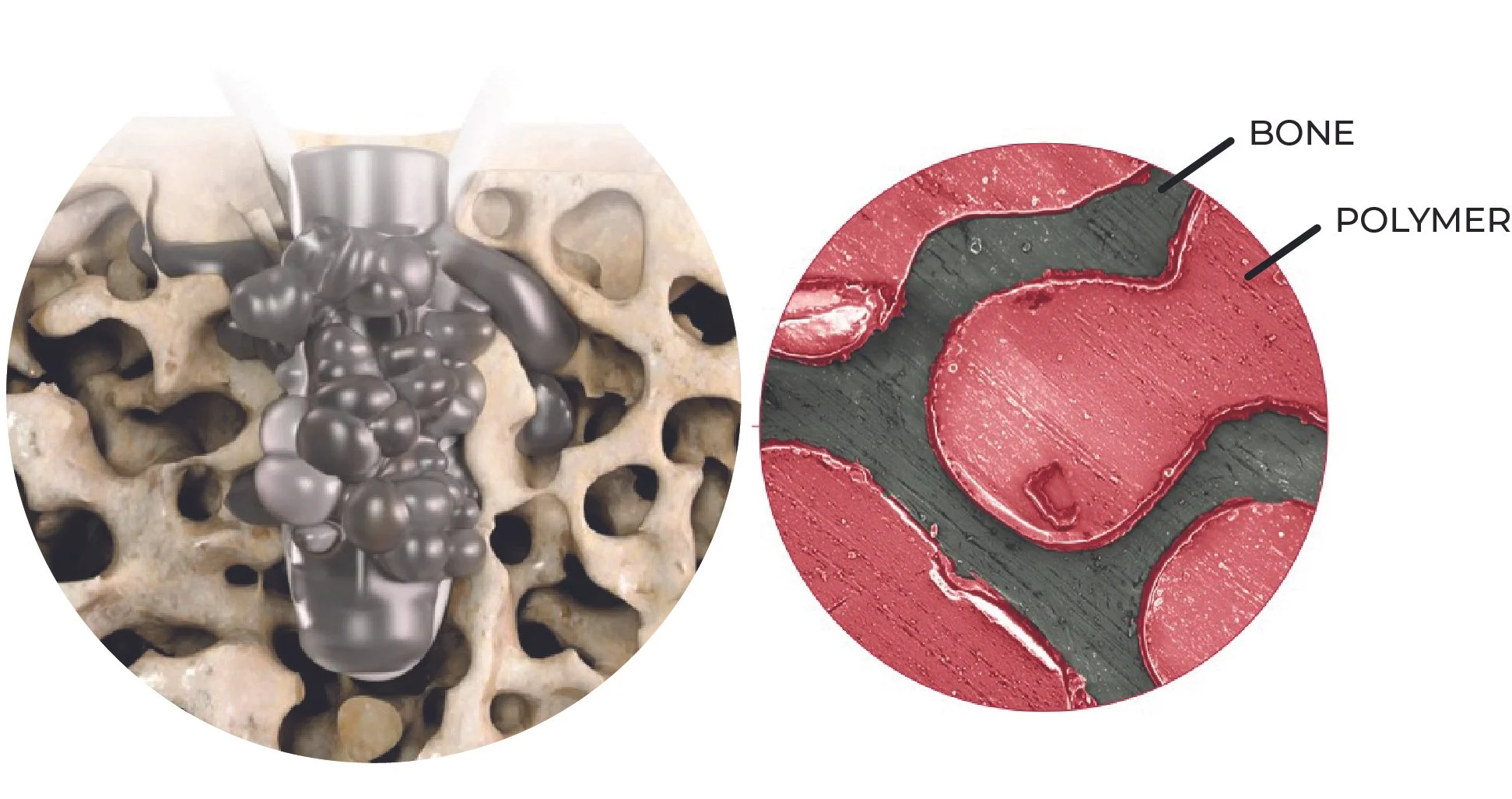
Figure 3: SF Push-in Anchor Augmentation. Ultrasonic liquefaction of the SF Push-in Anchor into the bone, without causing mechanical trauma, unlike conventional anchors.
Clinical Outcomes from a High-Demand Alpine Center
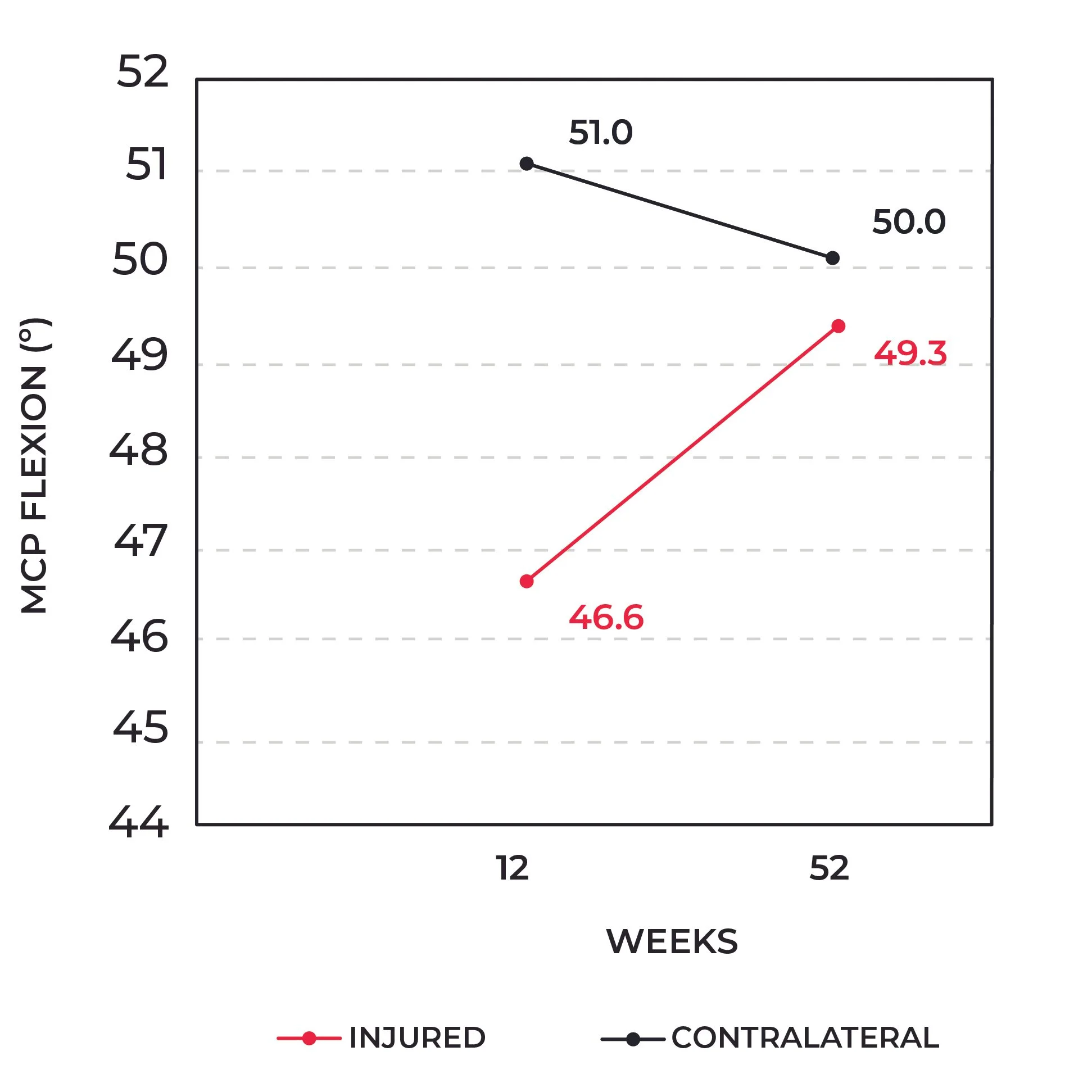
Figure 4: MCP Flexion. Range of motion in the metacarpophalangeal joint between the injured and contralateral thumb 12 and 52 weeks post-surgery.
Functional Recovery at 12 Months
In a prospective clinical series from Innsbruck, patients treated for skier’s thumb demonstrated:
MCP joint motion comparable to the contralateral side (Figure 4)
Grip strength between 79–100% of the uninjured thumb and a similar pinch strength as the uninjured thumb (Figure 5a, 5b))
Low pain scores and high satisfaction at final follow-up (Figure 6)
These results are particularly notable in the alpine trauma context, where patients often aim to return to skiing and other high-load activities that require confident grip and valgus stability.
This is where engineering thinking moves from analogy to application.
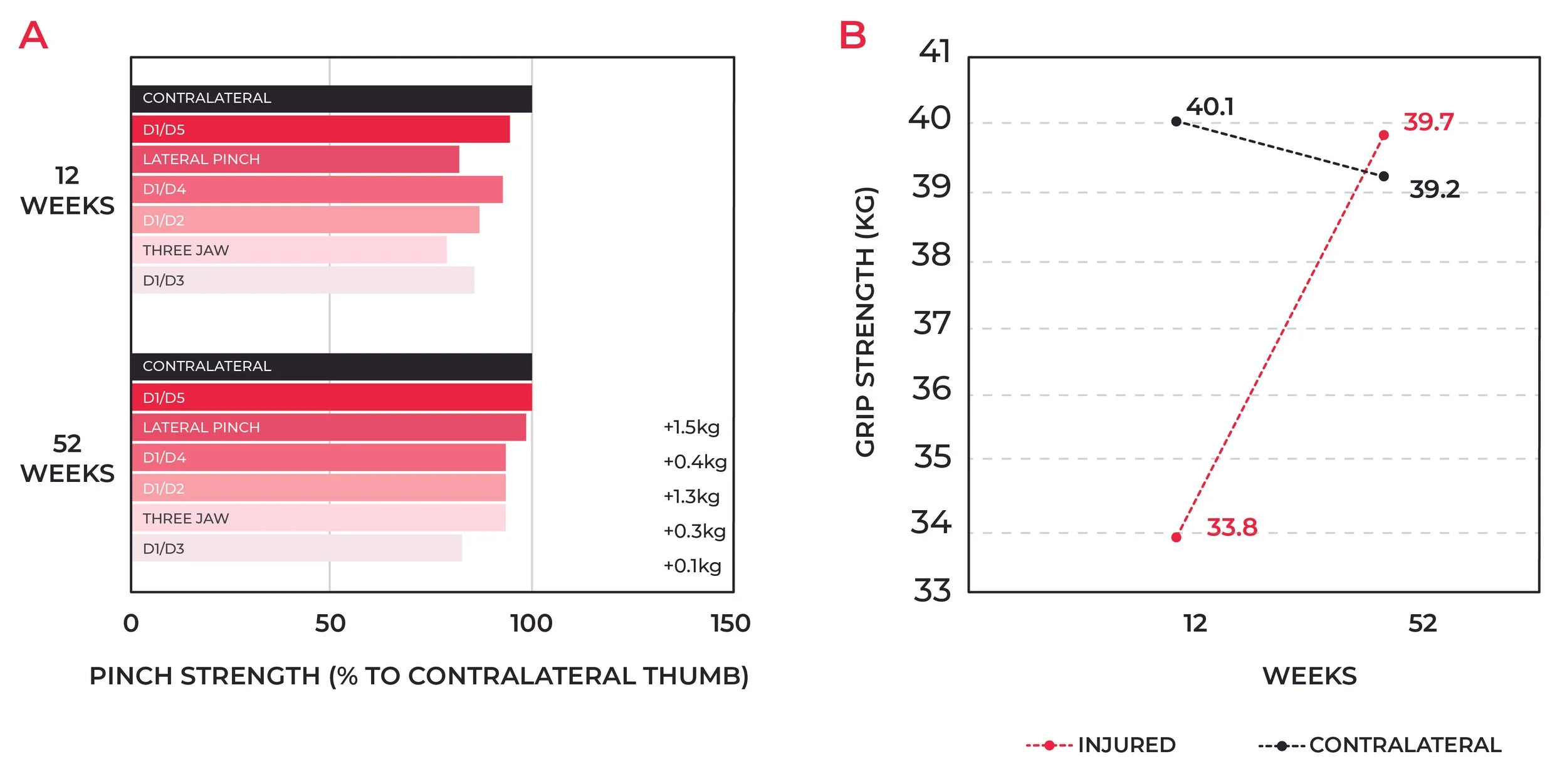
Figure 5: Pinch And Grip Strength. Pinch (a) and grip (b) strength 12 or 52 weeks post-surgery.
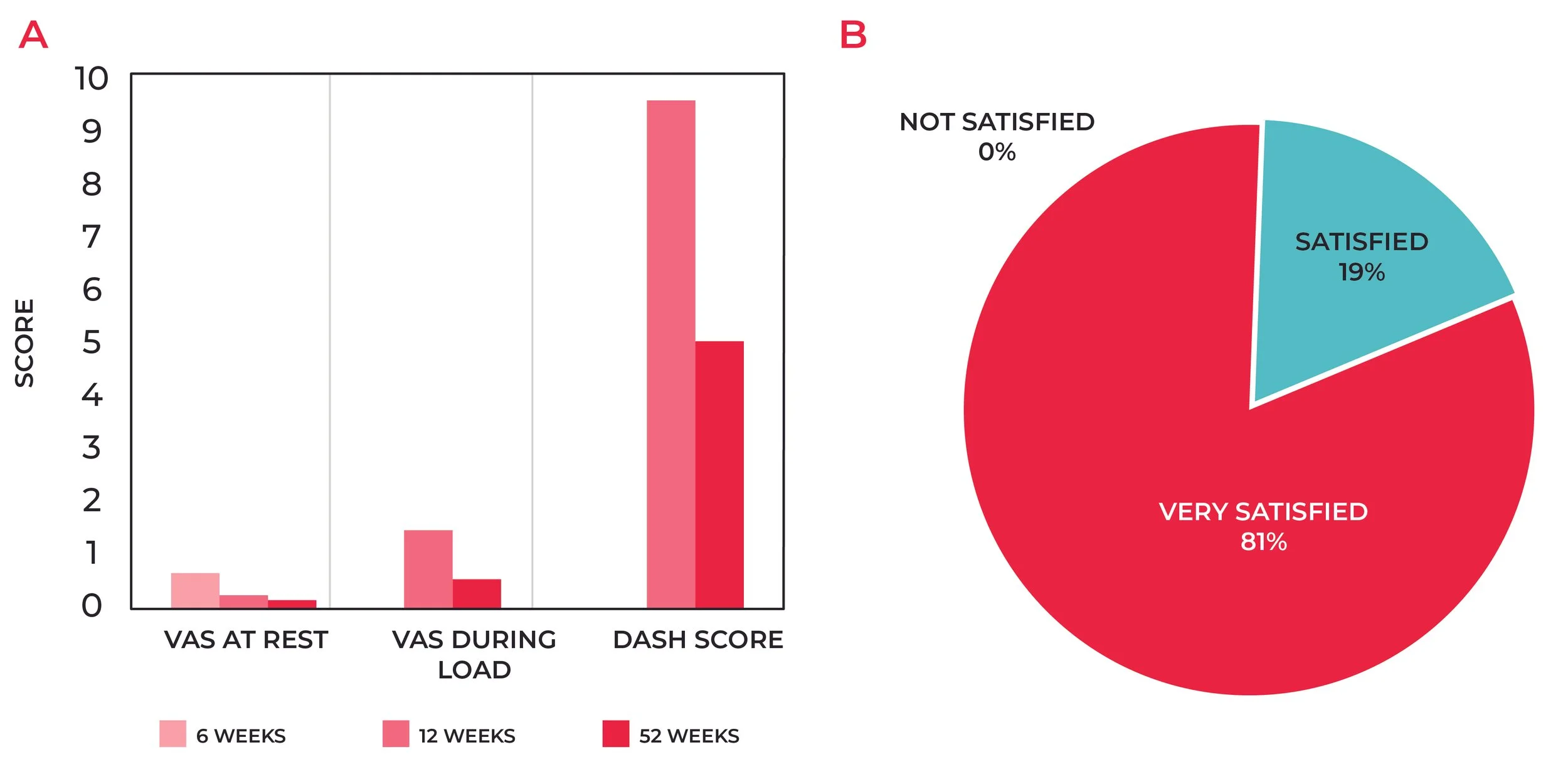
Figure 6: Pain, Dash Score, And Patient Satisfaction. Pain, Dash Scores (a), and patient satisfaction (b) 52 weeks post-surgery.
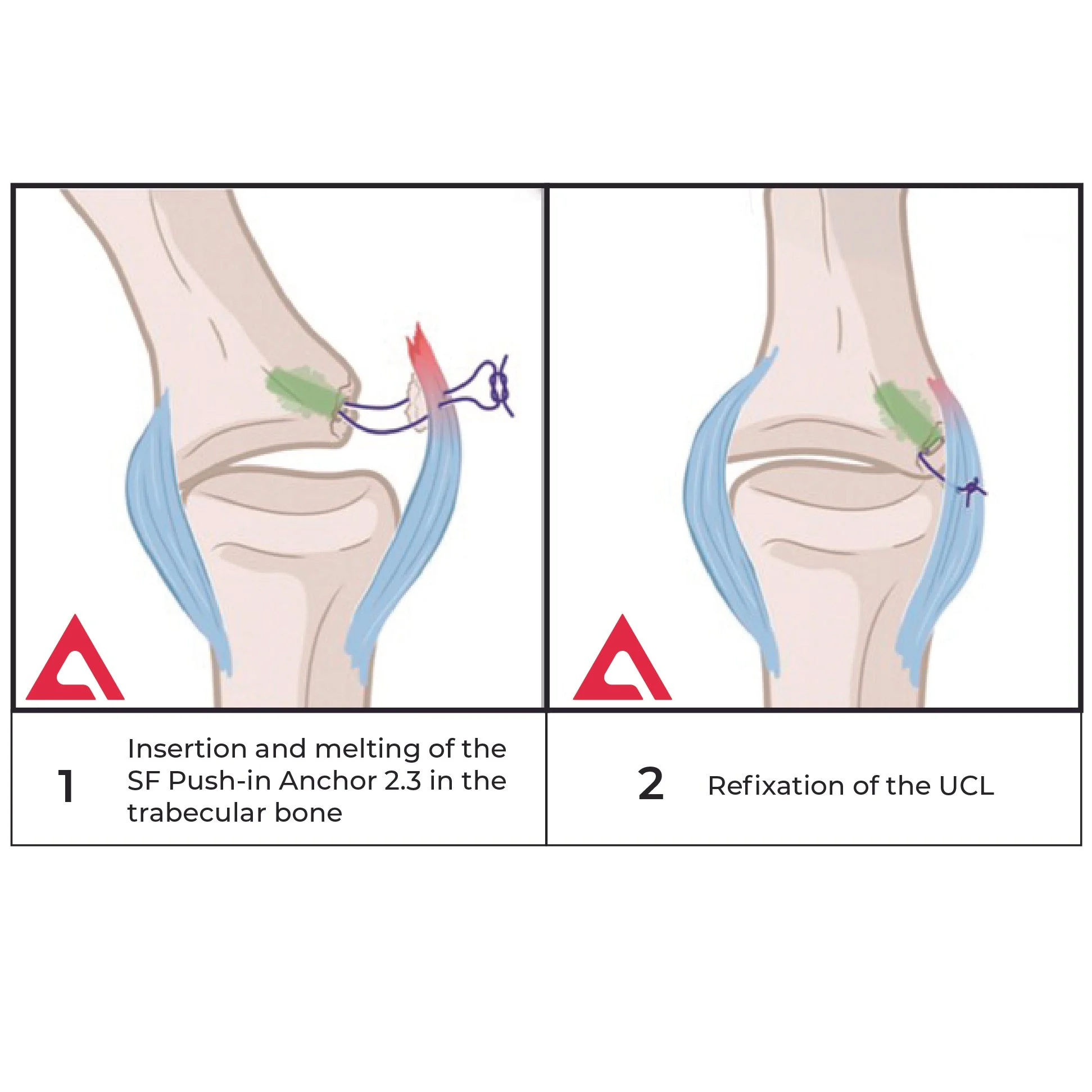
Figure 7: UCL Reattachment With SupraFusion. Reattachment of UCL at the small and delicate MCP joint with a small footprint 2.3mm SF Push-in Anchor.
From Challenge to Solution — SupraFusion Technology
SupraFusion Technology is designed specifically to address the constraints of small and delicate bone anatomy. With their minute dimensions, the SF Push-in Anchors minimize bone removal while leveraging ultrasonic energy to achieve intimate integration with cancellous bone.
Despite its minimal footprint, the system provides high fixation strength relative to size, enabling stable anchorage even in the absence of an intact cortical shell. This robustness directly supports the functional outcomes observed clinically: restoration of near-symmetrical strength, preserved range of motion, and low pain levels.
Broader Implications for Surgeons and Patients
For surgeons treating skier’s thumb, particularly in athletic or high-demand populations, fixation strategies must balance biomechanical robustness with anatomical preservation. For educated patients, understanding that successful repair is not just about healing but about restoring confidence, grip strength, and performance can help set realistic expectations.
The combination of small implant size, cancellous bone stability, and consistent clinical outcomes positions SupraFusion Technology as a compelling option when millimeters truly matter.
Key Takeaway
SupraFusion Technology implants are exceptionally small and specifically engineered for delicate bone anatomy, such as the thumb. Despite their minimal footprint, they achieve high fixation strength relative to their size, providing robust anchorage in cancellous bone, even in the absence of an intact cortical shell. This stability enables restoration of near-symmetrical strength, range of motion, and low pain levels, supporting a return to sport performance close to pre-injury with a minimal complication rate.
Explore how SupraFusion Technology can support stable thumb UCL repair at www.supra-fusion.com.
References
1. Wagner M, Schmoelz W, Stofferin H, Arora R. Biomechanical in vitro comparison of suture anchors for thumb ulnar collateral ligament repair.Archives of Orthopaedic and Trauma Surgery. 2018;138(3):435–442. doi:10.1007/s00402-018-2877-1.
2. Kastenberger T, Kaiser P, Schmidle G, Stock K, Benedikt S, Arora R. Clinical results of the BoneWelding® Fiji® anchor for the treatment of Stener lesions of the thumb.Archives of Orthopaedic and Trauma Surgery.2021;141(5):805–814. doi:10.1007/s00402-020-03625-x.